Rotator cuff repair
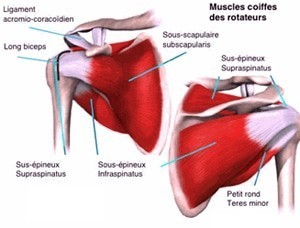
The rotator cuff is made out offive tendons (from front to back):
- subscapularis tendon;
- long biceps tendon;
- supraspinatus tendon;
- infraspinatus tendon;
- minor teres tendon
These tendons insert in the scapula and merge into a musculotendinous screed which covers the humeral head and fits into the greater and lesser tuberosities of the humerus. It then passes under an osteoligamentary vault formed by the acromion, the collarbone, and the acromiocoracoid ligament.
A – Non ruptured tendinopathy
These tendons may degenerate with age. This process usually starts at their weakest spot: the supraspinatus tendon insertion into the greater tuberosity of the humerus.
This degeneration may be hastened by different factors, such as excessive repetitive movements during sports or professional activity (painting, plastering, body-building, etc.) or by anatomical factors like the subacromial conflict.
This disease is common after 40 years of age. It manifests itself by pain that occurs first after effort and then becomes permanent, even during the night.
Clinical examination may provide some clues for the diagnosis. The patient will then undergo X-ray examination to assess the extent of the subacromial beak. An ultrasound may be instrumental in providing information on the rotator cuff’s condition. An important aim of the clinical examination is to exclude a ruptured rotator cuff syndrome.
Medical treatment consists of one or two corticosteroid infiltrations in the subacromial bursa in conjunction with proper rehabilitation.
In cases of non-response to a properly conducted 2-month medical treatment, arthroscopic surgery may be considered. An arthroscanner completes the assessment in order to exclude rotator cuff rupture.
The procedure involves settling a partial rupture and “raising the ceiling height” by planning down part of the acromion (anterior inferior acromioplasty). The intervention is conducted under arthroscopic control using a motorized drill, either under local or general anesthesia (or a combination of both).The procedure takes about 30 minutes and requires 2 days of rest. No postoperative immobilization is needed. Regular rehabilitation should be carried out.
B – Ruptured tendinopathy

Cette usure progressive de l’extrémité distale des tendons de la coiffe des rotateurs peut conduire progressivement à une rupture complète entraînant douleurs et perte de force.
Outre les signes de conflit sous-acromial, l’examen clinique va mettre en évidence des signes en faveur d’une rupture de la coiffe des rotateurs. L’arthroscanner ou l’arthro-IRM confirmeront ce diagnostic.
The progressive wearing of the extremities of the rotator cuff tendons may lead to a complete rupture, causing pain and loss of strength.
In addition to signs of subacromial conflict, the clinical examination may reveal signs in favor of a rotator cuff rupture, which will be confirmed via arthroscanner or arthro-MRI.
The decision to operate depends on the extent of the rupture, the patient’s age, (especially his physiological age), and the patient’s level of activity. Fixing a rupture is easier and gives better results (with less recurrence) if the rupture is not too extensive and if the muscles fibers have undergone only little fat degeneration.
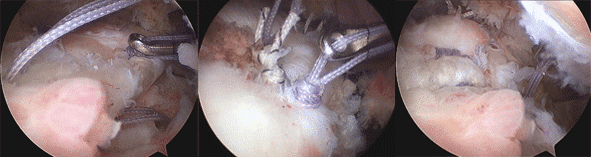
The procedure is performed under arthroscopic control and requires 48 hours of hospitalization. Absorbable anchors with suture threads are placed on the tuberosities. After avivement of the insertion area, the surgeon uses these threads to perform the reinsertion. An anterior inferior acromioplasty completes the procedure.
Following the surgery, the upper limb is immobilized with a splint for 6 weeks (abduction vest or elbow-to-body splint, depending on the rupture’s extent). For the patient it is important to conduct regular rehabilitation using passive joint amplitudes without any limitation. Complete active work will be authorized 6 weeks after surgery.
In addition to degenerative ruptures, there are traumatic ruptures that occur in patients without any significant past history, following severe shoulder trauma. The main symptom is sudden and severe pain. These traumatic ruptures of healthy and soft tendons quickly lead to severe retraction, rendering surgery difficult. They have to be taken care of and repaired as soon as possible, especially in young patients.
