Anterior Cruciate Ligament surgery (ACL)
1/ Anatomy
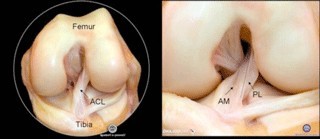
A ligament is a short strip of fibrous connective tissue made out of long collagen molecules. It is an extremely strong structure that ties the bones together within the joints. Ligaments control joints’ movements. They protect the joint in case of forced movements during a sprain. There are four main ligaments involved in the knee area: two lateral ligaments (internal lateral ligament and external lateral ligament) on each side of the knee, and two central ligaments called “cruciate,” as they cross in the middle of the knee: the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL).
2/ Diagnostis
The ACL is usually damaged following torsion or hyperextension. Patients may feel a snap, followed by swelling and unsteadiness of the knee. ACL lesion diagnosis is made based on knee examination and laxity measurements. These measurements are conducted using a device (arthrometer or GeNouRoB) or dynamic X-rays. Devices like the arthrometer (manual measurements) or the GeNouRoB (computerized measurements) measure the anterior displacement according to strength, compared to a healthy knee.
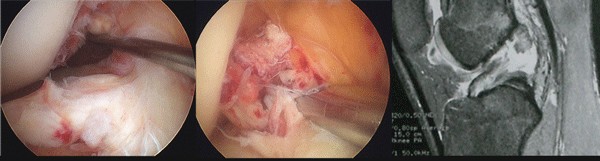
When the anterior cruciate ligament is damaged, this displacement is increased, reflecting an ACL injury. MRI helps visualizing the ACL rupture, but “false negatives” and “false positives” do exist. The MRI is mainly useful to assess the meniscal lesions.
3/ Suitability for surgery
In order to avoid accidents due to unsteadiness while playing sports, the surgeon and his patient will take the decision to operate on ACL, depending on different factors such as age, the intensity of physical activity, and associated professional duties. Episodes of unsteadiness can lead to a secondary tear of the meniscus, which, combined with the cruciate ligament rupture, is conducive of osteoarthritis. Early ACL reconstruction helps avoiding these secondary meniscal lesions, which is crucial in young patients.
We can distinguish three groups of patients:
– Young and active patients, for whom immediate ACL reconstruction is the best option, given the high risk of unsteadiness and meniscal lesion;
– Older and moderately active patients, who should have physiotherapy first, and only undergo surgery in the event of later unsteadiness;
– An “intermediate” group of patients will have their treatment decided according to their activity needs as well as their professional and personal duties. Some will be administered physiotherapy and only undergo surgery in case of later unsteadiness, while others will undergo surgery right away.
A short period of rehabilitation (a few weeks) is usually helpful prior to surgery, in order to prepare the knee in case of severe pain, stiffness, and swelling. On the other hand, when severe injuries to the lateral ligaments accompany the cruciate ruptures, operating immediately facilitates improved healing.
