Posterior cruciate ligament surgery (PCL)
A ligament is a short strip of fibrous connective tissue made out of long collagen molecules. It is an extremely strong structure that ties the bones together within the joints. Ligaments control joints’ movements. They protect the joint in case of forced movements during a sprain. There are four main ligaments involved in the knee area: two lateral ligaments (internal lateral ligament and external lateral ligament) on each side of the knee, and two central ligaments called “cruciate,” as they cross in the middle of the knee: the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL).
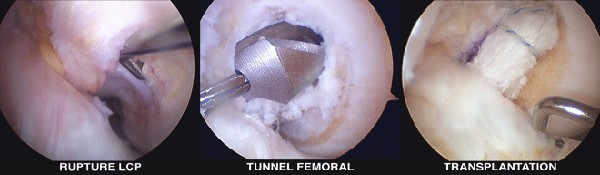
Rupture of the posterior cruciate ligament (PCL) is not a common injury, and is usually misdiagnosed due to good functional adjustment 85{88b696bf2700d12398c30964f41039de701ab1baffac505c8144f3e2e2571fd4} of the time (discomfort and pain during deceleration). Unlike anterior cruciate ligament ruptures (ACL), there is almost no unsteadiness. It is also a difficult surgery–all the more reason for neglecting this procedure over the years. Today, many authors insist on the long-term arthrosic potential of posterior laxity resulting from PCL ruptures. This is due to the increased stress on the patellar cartilage and internal tibiofemoral compartment. In recent years, research has allowed for improved procedures, thanks to better anatomical and biomechanical knowledge and advanced arthroscopy techniques.
At the acute stage, treatment is usually functional, not surgical. A physiotherapy program is scheduled. Surgery is indicated in cases of ruptures that lead to extreme posterior laxity, especially when combined with peripheral lesions. Posterior laxity has to be measured using dynamic X-rays. Later on, the need for surgery depends only on unsteadiness or a painful patellofemoral joint.
Au stade aigu, le traitement est le plus souvent fonctionnel, non chirurgical. Un programme de rééducation est mis en place. Une intervention chirurgicale est réservée à des ruptures responsables d’emblée d’une laxité postérieure très importante surtout si elle est associée à des lésions périphériques notamment des formations externes. La laxité postérieure différentielle doit être mesurée par des radiographies dynamiques.
Plus tard, la nécessité de cette réparation chirurgicale dépend uniquement d’une éventuelle instabilité ou plus souvent de douleurs de la fémoro-patellaire.
Les suites opératoires et la rééducation sont beaucoup plus difficiles et beaucoup plus longues que celles du croisé antérieur. Il peut persister une petite laxité postérieure résiduelle mais le résultat fonctionnel est en général bon.

