Shoulder instability
Shoulder instability is a common disease in young and active patients, and this condition may manifests itself in different ways: dislocation, subluxation, or simple pain when moving the arm.
Shoulder dislocation is usually a sports accident (skiing, practicing martial arts, surfing, playing hockey, etc.). In most cases, the shoulder dislocates itself outwards: anterior dislocation.
This condition is very painful and may be associated with coil fractures (in the youngest patients), humeral fractures (in older patients), or paralysis (circumflex nerve). If it occurs after 40 years, dislocation may lead to rotator cuff injury. These injuries, which are treated in the emergency room, may recur (recurrent shoulder dislocations), especially in young, active patients.
Diagnosis of shoulder anterior instability is easy, as the patient will describe his recurrent dislocations. X-ray examination often reveals visible marks, like blunt edges, remote fractures of the coil’s anterior inferior edge, or bone notches on the upper part of the humeral head (Hill-Sachs injury).
Patients without a real dislocation may present subluxation episodes or pain when moving the arm. In these cases, the arthroscanner or arthro-MRI may reveal a Bankart injury corresponding to a disinsertion of the glenohumeral ligaments, mostly of the inferior glenohumeral ligament on the coil’s anterior edge.
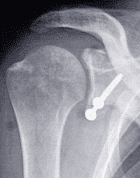
Surgical treatment may involve open surgery or arthroscopy.

- Open surgery consists of securing the coracoid process with two screws to the coil’s anterior inferior end.
- Arthroscopic surgery consists of freshening the detachment area and then reinserting glenohumeral ligaments with threads leaned on anchors into the bone.
Several factors such as the type of sport that is done, the extent of the instability and the presence of bone lesions will help deciding which technique should be used, in order to restrict the recurrence risk, which is higher with arthroscopic procedures.
When an arthroscopic reinsertion is done, the patient will have to wear a splint (elbow to body) for a month. For this procedure, as the joint stops are robustly secured, the splint can be taken off two weeks after surgery. The recovery of external rotation will be limited the first 4 weeks to avoid stress on sutures.
