Knee prostheses
The first knee prostheses were developed about 30 years ago and changed the lives of many patients who could barely walk without pain. Placing knee prosthesis should be considered when pain, disability or effusions get worse, and medical treatments (anti-inflammatory drugs, infiltrations, viscosupplementation) are ineffective to the point where standing up, going upstairs, and walking become a problem. The patient has to decide according to his level of disability.
The surgeon can either replace the entire knee or part of the articular surfaces on the femur, tibia, and patella with a prosthesis made out of two to three different implants:
The femoral prosthesis (made out of chromium and cobalt) will slide on the polyethylene tibial plateau.
The tibial prosthesis comprises two parts:
- a metal plateau made out of chromium and cobalt or titanium and anchored to the tibia
- a polyethylene plateau resting on the tibial metallic plateau. This plateau can be either fixed or rotational. It ensures friction between the tibia and the femur.
The kneecap polyethylene prosthesis is only used when the patellar cartilage is severely worn-out.
Placing a prosthesis is a very common, well-standardized procedure, which usually takes 1 hour to 1.5 hours, depending on possible complications during surgery.
Placing knee prosthesis can be done using computerized monitoring, which allows for accurate positioning of the prosthetic parts.
The application system can be tailor-made based on MRI data obtained prior to the procedure. A “navigation” system can also be used.
Postoperative pain is managed using strict pain control protocols and by inserting a catheter at the root of the thigh in order to insure postoperative analgesia.
Anticoagulation and support stockings are prescribed so as to prevent phlebitis.
1- Unicompartmental knee arthroplasty
If the knee damage is limited to the joint’s inner side or to its outer side, the injured part’s articular surfaces can simply be replaced.

Single compartment prostheses are indicated in the following cases: The injury is limited to one of the tibiofemoral compartments (the other compartments are healthy), the cruciate ligaments are intact, the body mass index is below 30, there is no stiffness in the knee, and the deviation is less than or equal to 15°.
As previously mentioned, this prosthesis includes a femoral implant, a tibial implant, and a pad that only replace “half of the knee.”
Incisions and the surgical approach in general are less invasive than a few years ago, thanks to improvements in equipment and procedure. These new techniques are called minimally invasive surgeries (MIS).
This procedure involves a skin incision (6-8cm), an opening of the knee without cutting tendons or muscles more than 1cm, spreading the patella without reversing it, and equipment adapted to this minimally surgical approach.
This procedure facilitates faster recovery and decreases pain and bleeding.
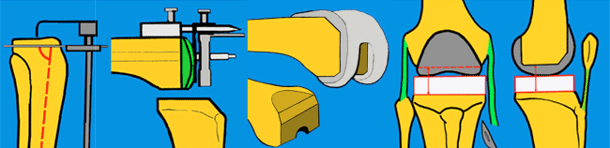
Once the bone slices are made and the trial implants placed, ligament balance and stability during knee flexion are checked.
All of these benefits combined with pain control protocols allow for easier postoperative recoveries and shorter hospitalization periods.
2 – Tolal knee arthroplasty
- This type of prothesis completely replaces the joint, except for the patella, which can be left without putting a polyethylene button prosthesis (provided the cartilage is still in good condition).
Aside from the joint reconstruction, the procedure allows for the reduction of preoperative deformations (varus or valgus on the lower limb).
Ligament balance and stability and patellar alignment are checked once the bone slices are made and the trial implants are placed. Kneecap resurfacing through a polyethylene button is not mandatory.

Patients’ blood is recovered during and right after surgery (Cell Save), which reduces the need for blood transfusions. Your blood is recovered during and right after surgery (Cell Saver) which reduces transfusions.
