Patellofemoral Disorders
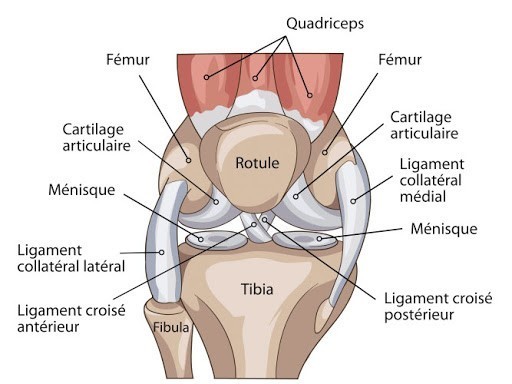
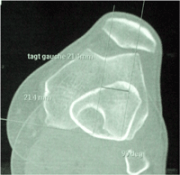
The patella is located on the anterior part of the joint, between the quadriceps tendon and the patellar tendon, which is attached to the anterior tibial tuberosity (ATT, spina tibiae). Its surface connects with the femur’s trochlea, which is hollow so the kneecap stays centered during knee movements. It is drawn outwards by traction from the quadriceps and the external retinaculum, and by the discrepancy between the ATT axis and the trochlea’s neck axis (TA-GT). It is held inwards by the vastus medialis muscle, and the medio patellofemoral ligament.
Bone malformations (trochlea is not hollow enough, ATT is severely off-centered) or poor tension of these elements increases patellar instability.
 Surgical repair of the patella often requires several combined procedures. It is convenient to distinguish two groups: procedures that correct bone anomalies, and procedures that correct anomalies on soft parts.
Surgical repair of the patella often requires several combined procedures. It is convenient to distinguish two groups: procedures that correct bone anomalies, and procedures that correct anomalies on soft parts.
If there is no instability, the patellofemoral joint may “only be painful.” This pain is exacerbated by anatomical anomalies similar to patellar instability.
In this case, treatment will be medical at first (rehabilitation, insoles, knee support, intra-articular injections). If medical treatment is unsuccessful, surgery may be considered.
Bone corrections
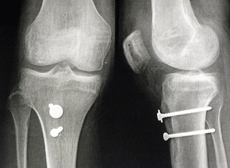
Transposition of the anterior tibial tuberosity is a procedure that realigns and pulls down the off-center kneecap. The tibial tuberosity is removed and screwed inwards and/or lower. Trochlear recession is performed in order to improve patellar stability by hollowing out the flat trochlea, making it concave, and facilitating proper kneecap retention. These procedures are not common, and should be reserved for cases of severe trochlea dysplasia (convex trochlea).
Patellofemoral ligaments surgery
 Patellofemoral ligaments surgery can be performed alone if there are few bone anomalies, or it can be combined with ATT transposition.
Patellofemoral ligaments surgery can be performed alone if there are few bone anomalies, or it can be combined with ATT transposition.
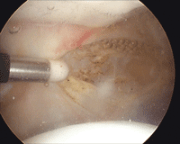
If the kneecap is painful and only barely unstable, we cut the external retinaculum and tighten the internal retinaculum with subcutaneous stitches through arthroscopy.
A new procedure was developed a few years ago in order to treat severe patellar instabilities. It is a reconstruction of the medial patellofemoral ligament that uses the gracilis tendon (MPFL: Plasty). The gracilis tendon is taken with a stripper (as for ACL surgeries). It is secured with two absorbable anchors to the kneecap’s inner edge, and then both ends are tightened in a tunnel by an absorbable screw on the inner edge of the inner condyle. There are only three incisions, 1cm long. The patient stays at the hospital for 48 hours, after which he walks with a crutch and a splint for 3 weeks.
Resumption of sports is possible 3 months after the surgery.
This new procedure is very interesting, as it is non-invasive and effective as far as patellar
