Knee anatomy and pathophysiology
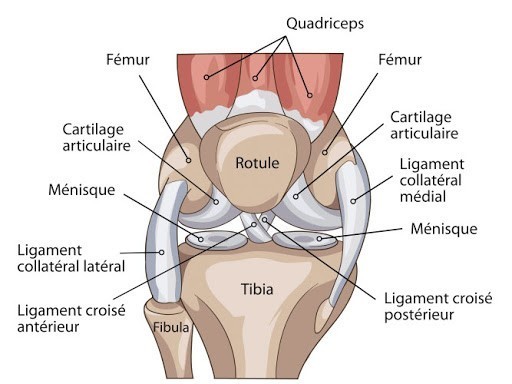
The knee joint is the junction between the tibia and the femur. On a functional level, it is the most complex joint in the human body, and comprises three bones: the femur, the tibia, and the patella, hold together by three joints: the patellofemoral joint and the double tibiofemoral joint.
Cartilage (a thin, elastic tissue) allows for fluidity in the knee’s movements. It protects the bone and makes sure the joints’ surfaces slide easily against each other. The knee contains two types of articular cartilage: the fibrous cartilage (meniscus) and the hyaline cartilage. Cartilage wears out as time passes and with use. Its ability to regenerate is limited due to the absence of blood vessels. In the event of a lesion, the replacement scar tissue is made out of fibrous cartilage, a low-grade substitute for the original hyaline cartilage. The cartilage layer may continue to wear out, resulting in osteoarthritis.
These degenerative lesions are the most common cause of osteoarthritis, although they may be caused by injuries that occurred in young and active patients. This wear and tear can be enhanced by different osteoarthritis-inducing factors (repeated micro-traumatisms, overweight, varus or valgus lower limb deviation, chronic and long-established loose-jointedness, as well as traumatic after-effects from fractures of the joint surfaces), or by local diseases (aseptic osteonecrosis of a femoral condyle), or systemic diseases such as inflammatory rheumatisms.
The joint is enveloped by a synovial membrane, which is responsible for the production of synovial fluid. This membrane may be the site of inflammation due to joint dysfunction (meniscal injury, cartilage degradation, etc.) or disease states (benign tumor on the synovial membrane, such as villonodular synovitis or osteochondromatosis).
